Shenzhen Doctor Consultation — 2026-05-24
Date of consultation: ~May 24, 2026 Consulting physician: Dr. Chen (陈主任), Shenzhen Second People's Hospital (深圳二院) Other physicians referenced:
- Dr. Wu (胡医生) — Hong Kong, mom's current treating doctor; made the referral to Tiantan and Shenzhen, and prescribes TMZ in HK
- Prof. Ren / Ren Xiaowei (任小威教授) — Tiantan Hospital (天坛医院), Beijing, the doctor who pushed back on penetration therapy
TL;DR
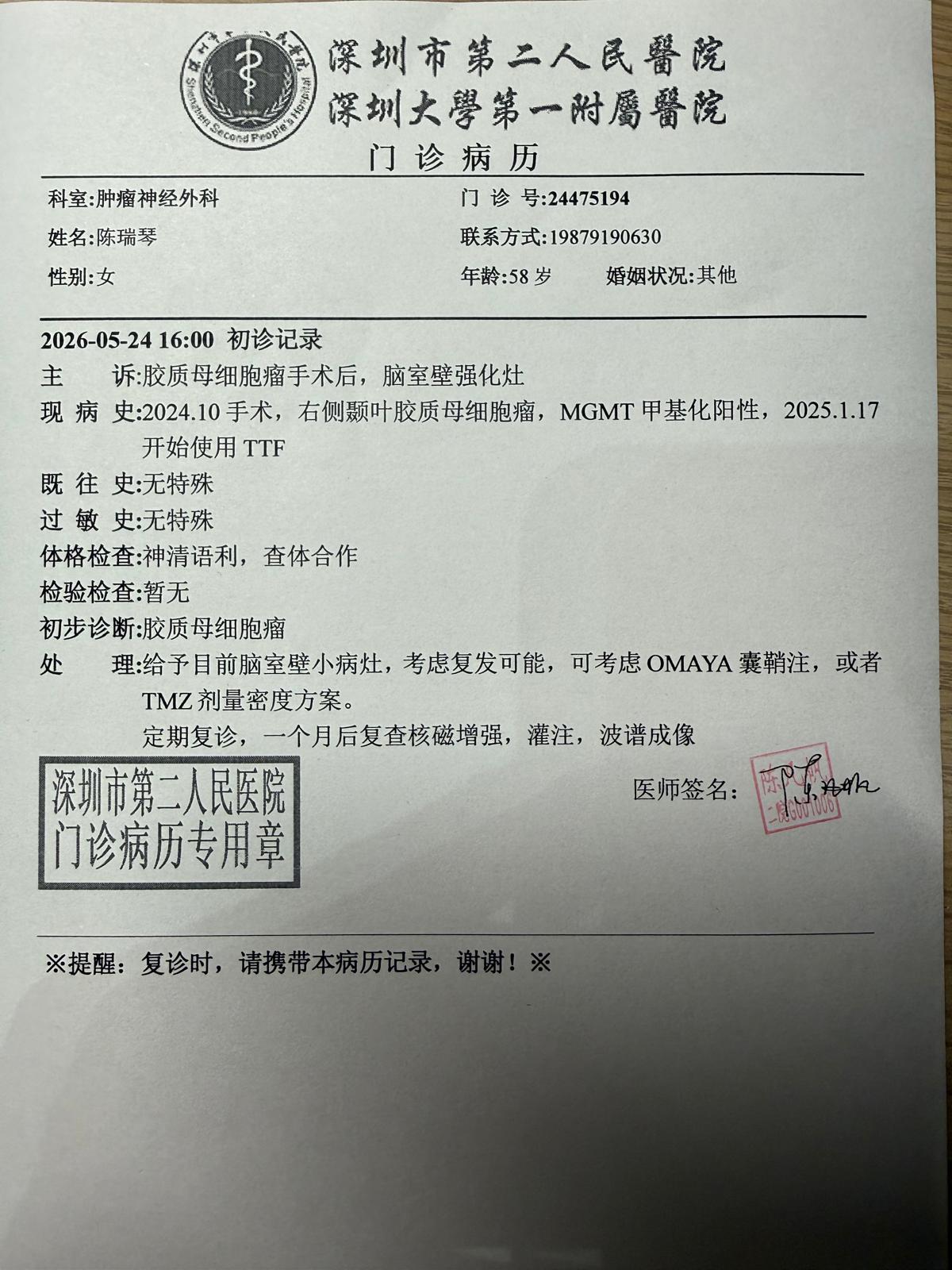
Dr. Chen's working diagnosis: most likely tumor recurrence with a risk of dissemination through the cerebrospinal fluid (CSF). A new enhancing lesion has appeared on the ventricle wall, in a location remote from the original tumor site, and it has grown between the February and April MRIs — and because the original tumor was attached to the ventricle wall, CSF dissemination is a known pathway. Pseudo-progression cannot be fully ruled out (mom is MGMT methylation positive and on TTF, both of which elevate that rate), which is why the recommended first step doubles as a diagnostic test.
Both Tiantan and Dr. Chen agree against starting bevacizumab-based "penetration" therapy now, because bevacizumab will visually erase the lesion and make it impossible to know whether the chemo is actually working. The recommended path is a stepped, lowest-invasiveness-first plan:
- First: Dose-dense temozolomide (TMZ rechallenge) — daily low-dose oral. Monthly MRI to monitor.
- If TMZ fails (lesion grows AND high perfusion on MRI): Ommaya reservoir implant + intraventricular methotrexate (MTX) — Tiantan's proposed approach.
- Last resort: Penetration therapy (TMZ + kinase inhibitor + bevacizumab).
Continue TTF (Optune patches) throughout.
Doctor's note from the consultation
1. Why Tiantan Hospital does NOT recommend "penetration" therapy
What penetration therapy is: A three-drug combination regimen:
- Temozolomide (替莫唑胺, TMZ) — oral chemo
- A second agent (transcribed as 博莱替尼; likely a targeted/kinase inhibitor)
- Bevacizumab (贝伐单抗, Avastin) — anti-VEGF antibody
Tiantan's objection — the "pseudo-response" problem caused by bevacizumab:
- Bevacizumab works partly by shrinking blood vessels and reducing contrast enhancement on MRI. Once it's used, every enhancing white lesion on the MRI will visually disappear — whether or not the chemo is actually killing the tumor.
- This means you lose the ability to tell whether the chemo (TMZ + the second drug) is doing anything, because bevacizumab masks the imaging signal that lets you measure response.
- Dr. Chen's words: "you all the enhancing lesions, the white ones, disappear — but you don't know if it's the temozolomide + [kinase inhibitor] working, or just bevacizumab. You can't distinguish whether it's actually effective."
Tiantan's counter-proposal: Ommaya reservoir + intraventricular methotrexate
- Implant a small reservoir (Ommaya/奥美亚囊) under the scalp.
- Inject methotrexate (MTX) directly into the ventricle via the reservoir.
- Rationale:
- The recurrence lesion sits on the ventricle wall, and CSF circulates through the ventricles — so MTX delivered directly into the ventricle bathes the lesion.
- MTX is a true tumor-killing drug, not a masking agent — so you can actually measure response on MRI.
- Avoids spending the "bevacizumab card" too early. Bevacizumab is best saved for later when edema is severe and quality of life is suffering (its anti-edema effect is genuinely useful then).
Dr. Chen's verdict on Tiantan's reasoning: "I think it's reasonable. Prof. Ren's logic is sound."
2. Dr. Chen's recommended options (and why)
Dr. Chen proposes a two-option fork, with a clear order of preference:
Option A (recommended first): Dose-dense TMZ rechallenge
What it is: Switch from the old 5-day/cycle TMZ pulse to daily continuous low-dose TMZ.
Why this first:
- Mom is MGMT methylation-positive (甲基化阳性) — this means TMZ is significantly more likely to work for her than for the average GBM patient.
- She has been off TMZ for ~3 months (last dose February), so a rechallenge is medically appropriate ("team protocol rechallenge").
- It is the most convenient, lowest-pain, most acceptable treatment — no surgery, no hospital stay.
- It doubles as a diagnostic test: if the lesion shrinks/disappears AND perfusion is low on follow-up MRI, you've also confirmed the lesion was likely pseudo-progression — not true recurrence.
Option B (if Option A fails): Ommaya reservoir + intraventricular MTX
This is the Tiantan-recommended approach, which Dr. Chen would perform.
Option C (last resort): Penetration therapy (TMZ + kinase inhibitor + bevacizumab)
Only if Option A and B are exhausted or ineffective.
Why this stepped approach
Dr. Chen's framing: "There's no scientific data comparing these three side by side — no paper says A is better than B is better than C. So we go with the most acceptable option first, watch, and escalate if needed. 'Side by side, you can't say one is definitely good and one is definitely bad. Whichever path you take, we walk and watch.'"
3. Procedures and precautions for each treatment
Option A — Dose-dense TMZ
Dosing:
- Previous regimen: 280 mg/day × 5 days/cycle = 1,400 mg per cycle
- New regimen: 60–80 mg/day, every day, for one month
- At 60 mg × 30 days = 1,800 mg/month (~400 mg more than before)
- At 80 mg × 30 days = 2,400 mg/month (~800 mg more than before)
- Total monthly drug exposure is higher, but each day's dose is much lower.
Logistics:
- Need to get TMZ prescription from Dr. Wu in Hong Kong in dose-dense form. If HK won't prescribe dose-dense, get it from Shenzhen.
- Dr. Chen will provide WeChat contact of his assistant (Zhang) to help coordinate sourcing in HK or Shenzhen.
Monitoring & precautions:
- Monthly MRI (not every 3 months — Dr. Chen
explicitly corrected mom on this).
- When the follow-up MRI is done in Shenzhen, request advanced sequences: thin-slice contrast + perfusion + spectroscopy — these are needed to distinguish pseudo-progression from real recurrence.
- HK MRI does not reliably provide perfusion/spectroscopy sequences, and HK only releases printouts/CDs, not films — Shenzhen Second can't read CDs reliably. Do MRI in Shenzhen when escalation decisions are pending.
- Blood counts and liver function must be checked more frequently (higher total monthly drug exposure means more myelosuppression and hepatotoxicity risk).
- Continue TTF (Optune patches) as is.
Decision tree based on MRI findings:
| MRI finding | Interpretation | Action |
|---|---|---|
| Lesion shrinks or disappears | TMZ working OR pseudo-progression | Continue TMZ |
| Lesion grows, low perfusion | Pseudo-tumor (假肿瘤), not real recurrence | Continue TMZ |
| Lesion grows, high perfusion | True recurrence | Escalate — strongly consider Tiantan's MTX (Option B) |
Option B — Ommaya reservoir + intraventricular MTX (methotrexate, 甲氨蝶呤)
This is a two-part treatment: (1) one-time surgical implantation of the reservoir, then (2) a long-running schedule of MTX injections delivered through the reservoir. The surgery is the easy part. The MTX schedule is the hard part — it forces inpatient stays in mainland China and a rotation between multiple hospitals. Detailed breakdown below.
B.1 — The implantation surgery
What's implanted: An Ommaya reservoir (欧迈亚/奥美亚囊) — a small dome-shaped capsule placed under the scalp with a thin catheter that runs down into the ventricle. Once it's in, MTX can be injected into the reservoir from outside the skull, and the drug flows through the catheter directly into the cerebrospinal fluid.
Anesthesia: Local anesthesia only. Dr. Chen: "I can chat with you while doing it — as long as you're not scared. Cut open, place it in, sew it up. Twenty to twenty-five minutes."
Duration: ~20–30 minutes, start to finish.
Complexity: Dr. Chen explicitly described it as not a complex operation ("本身不是很复杂的一个手术"). It's a minor neurosurgical procedure — a small incision, place the reservoir in the subcutaneous space, thread the catheter into the ventricle, close up.
Placement and TTF patch coordination:
- The reservoir will be implanted in the empty space adjacent to / between the existing TTF (Optune) patches on her scalp.
- The TTF patch arrangement will need a small repositioning adjustment so that the patches don't sit directly on top of the reservoir site.
- This means: she will need to keep using TTF, and the patch layout gets reshuffled around the new reservoir location.
Precautions and recovery: Not explicitly covered in the consultation. Standard Ommaya post-op precautions to confirm with Dr. Chen at the time:
- Watch the surgical site for infection (Ommaya infection is the major late complication).
- Keep the scalp clean and dry until healed.
- Hair near the incision site will likely need to be shaved — Dr. Chen alluded to this in passing.
B.2 — The MTX injection schedule
The drug: Methotrexate (MTX, 甲氨蝶呤) — a real cytotoxic chemo agent. Delivered directly into the ventricle via the reservoir.
Three-phase tapering schedule (Dr. Chen's exact words):
| Phase | Frequency | Duration | Total injections |
|---|---|---|---|
| Phase 1 — Intensive | Every 3 days | ~1 month | ~10 injections |
| Phase 2 — Consolidation | Once a week | ~1 month | ~4 injections |
| Phase 3 — Maintenance | Once a month | Long-term, indefinitely | ongoing |
- Phase 1 starts very soon after the surgery — Dr. Chen said: "the day after surgery — day 2 or day 3 — we start injecting."
- The first ~6 doses in Phase 1 can be given during the post-op admission (4–6 doses in ~1 month), then continue in subsequent stays.
Each individual injection:
- Takes only a few minutes of actual injection time.
- Dr. Chen: "打就是几分钟" / "其实打得很快" — the injection itself is fast.
- The slowness/inconvenience is not the injection — it's waiting for a doctor with time to do it. "打就是出院,打,然后看那个 — 但是最主要是等医生."
B.3 — Why hospitalization is mandatory for every injection (Dr. Chen explained this in detail)
This is the most counterintuitive part. You'd assume MTX injection through a reservoir is a quick clinic visit. It is not, in this hospital system.
Dr. Chen's reasoning:
- Doctor availability. Dr. Chen personally performs ~20–30 brain tumor surgeries per month. "You think the doctor is so exhausted — you come from Hong Kong, and I'm also supposed to inject your drug? At 10pm, 11pm, midnight the doctor hasn't come down from surgery yet, and tomorrow there's another operation." MTX injections must fit into whatever gaps appear in his surgical schedule, which is unpredictable.
- Walk-in injections cannot be billed properly. "And you still can't be billed for the visit, honestly." Outpatient walk-in MTX administration isn't a recognized billable encounter at this hospital — so the hospital has no operational pathway for it.
- Both of the above mean: the only way to actually get the injections done is to be admitted as an inpatient, then wait for the doctor to have an opening between surgeries.
The result is a system where the drug is fast but the logistics force inpatient admission every time.
B.4 — Length of stay limits and inter-hospital rotation
This is the part that genuinely complicates the plan:
- Per-admission stay limit at Shenzhen Second: Hospital policy caps a typical inpatient stay at 10–14 days (Dr. Chen: "我这里的病人从入院到出院虽然大概是十天左右,十天到十四天").
- Maximum doses Dr. Chen can give in one stay: 3–6 injections. At 3-day intervals, 6 doses = 24 days, which already exceeds the 14-day ward cap. So in practice she'll get 4–6 doses per admission, ~1 month per admission cycle.
- After hitting the stay cap, she must transfer to another hospital to continue. Dr. Chen's plan: "From here you transfer to General Hospital (总医院). After General Hospital, possibly transfer to another outside hospital. After that, possibly back here. That's how it goes."
- Why he can't bend the rules: Hospital metrics enforce stay length. Dr. Chen said his cancer inpatients are already a "very, very small" cohort and "I have to use other patients to balance out the data" — i.e., he can already only barely accommodate Mom under hospital length-of-stay rules.
- Dr. Chen's personal commitment: "Since Prof. Ren personally spoke for you, I will absolutely take you on. I'll find a way to arrange this for you." He will personally coordinate the inter-hospital transfers.
B.5 — Why this can't be done in Hong Kong (or as a Shenzhen day-trip)
- Hong Kong does not do intraventricular MTX via Ommaya. Dr. Wu has confirmed this — the Hong Kong system isn't willing to perform these injections.
- She cannot go home between doses. At 3-day spacing in Phase 1, traveling back to Hong Kong between every injection is not feasible (border, travel time, drug schedule too tight).
- She cannot do this as a walk-in patient at Shenzhen Second. Per B.3, the hospital does not have a workflow for that.
- Net effect: during the intensive 2-month period (Phases 1+2), she will be living in mainland Chinese hospitals, rotating between Shenzhen Second → General Hospital → another hospital → back.
- Once she reaches Phase 3 (monthly), the cadence is relaxed enough that one trip a month from HK to Shenzhen for a short admission should be workable.
Direct cost commentary from Dr. Chen: Aside from the drug itself, the per-stay cost is "a few yuan" for accommodation — the financial burden is small, but the time and logistical burden is the real cost.
B.6 — Combining with oral TMZ during the MTX course
- Continue oral TMZ on the standard 5-day pulse cycle alongside MTX. (The daily dose-dense TMZ regimen from Option A is not used in parallel with Option B.)
- Take the TMZ on the same day as the first MTX injection of each cycle.
- Dr. Chen explicitly said the timing alignment is not critical — "这个没关系" / no need to be exact."
B.7 — Summary: pros and cons of Option B vs Option A
| Dimension | Option A (Dose-dense TMZ) | Option B (Ommaya + MTX) |
|---|---|---|
| Invasiveness | Oral medication only | Minor surgery + recurring injections |
| Living situation | Home life unchanged | ~2 months living in mainland Chinese hospitals, rotating between 2–3 hospitals |
| Cadence of medical visits | Monthly MRI in Shenzhen | Continuous inpatient for Phase 1–2; monthly trips for Phase 3 |
| Direct drug efficacy on this lesion | Systemic — works because she's MGMT methylation positive | Local — bathes the ventricle wall lesion in chemo directly via CSF |
| Cost (direct) | Drug only | Drug + accommodation (modest) |
| Cost (time/disruption) | Low | Very high during Phases 1–2 |
| When to choose | First-line, given MGMT+ status and 3-month TMZ washout | If lesion grows on MRI and is high-perfusion → true recurrence confirmed |
Option C — Penetration therapy (TMZ + kinase inhibitor + bevacizumab)
- Not discussed in procedural detail in this consultation — it's positioned as the fallback if A and B are exhausted.
- The doctor noted there are also clinical trials available, but most international ones exclude HK residents; some HK-specific trials may be accessible. To be discussed at the time.
4. Doctor's diagnosis of the current situation
Current clinical picture (as of May 24, 2026):
- Status: ~1.5 years post-resection (surgery was October 2024). Original tumor was adjacent to/connected with the ventricle wall.
- Treatment so far: TMZ × ~1 year (stopped February 2026); TTF (Optune) started Jan 17, 2025, ongoing.
- MGMT methylation: Positive (favorable — better TMZ response, also higher pseudo-progression rate).
- MRI findings (April 29 scan):
- New enhancing lesion on the ventricle wall, in a remote location from the original tumor site.
- Compared to February 2 MRI which already showed a small spot, the April 29 scan shows the lesion is larger and more pronounced.
Working diagnosis: Most likely recurrence with risk of dissemination (复发或播散).
Reasoning:
- Anatomic risk factor for dissemination: The original tumor sat on the ventricle wall, so surgery necessarily opened the ventricle. CSF can carry tumor cells to remote sites along the ventricular wall — this is a known dissemination pathway, and the new lesion's location is consistent with it.
- Time course: Nearly 2 years post-op is a typical window for GBM recurrence.
- Lesion is likely outside the original radiation target field — Dr. Chen looked at the imaging and judged the new spot is at or just past the edge of the radiation field. So this is not radiation necrosis.
- Pseudo-progression cannot be fully ruled out,
because:
- MGMT methylation-positive patients have higher pseudo-progression rates.
- TTF use also increases the rate of pseudo-progression-like imaging changes.
- The way to disambiguate is MRI perfusion: low perfusion → pseudo; high perfusion → real tumor.
Why the diagnosis matters for treatment choice:
- If this is pseudo-progression, no aggressive escalation is needed — TMZ rechallenge alone is enough.
- If this is true recurrence + dissemination, the MTX-via-Ommaya approach becomes the right tool (direct CSF chemotherapy).
- The dose-dense TMZ trial serves as a diagnostic step too: continued growth + high perfusion after 1–2 cycles confirms true recurrence and justifies surgery for the Ommaya reservoir.
Action items / next steps
Caveats
- These notes are reconstructed from two overlapping audio transcripts of the same consultation. Some Chinese medical terms in the transcripts were mistranscribed by the speech-to-text model (e.g., "GTF" should be "TTF"; "假句话" should be "甲基化" / methylation; "博莱替尼" is a kinase inhibitor whose exact identity should be confirmed with Dr. Chen).
- This is a layperson's summary, not medical advice. Please confirm all dosing, scheduling, and clinical interpretations with Dr. Chen and Dr. Wu before acting on anything.